
Patients who had a nerve block experienced good pain control during procedure, but some sought follow-up care for ongoing pain
Surgery for a distal radius fracture — also known as a broken wrist — is a common procedure, but how to manage pain in the days after surgery remains a matter of debate. New Kaiser Permanente research sheds light on the issue but is not likely to be the last word.
In a study published in the journal Regional Anesthesia and Pain Medicine, researchers reported on outcomes during the 7 and 30 days after distal radius fracture surgery among 5,635 adult patients at Kaiser Permanente Northern California between January 2017 and December 2022.

Of these, two-thirds received regional anesthesia, in this case a brachial plexus nerve block focused on numbing the arm. The other third did not have a nerve block, but received a different combination of sedation and pain control medication.
The nerve block appeared to have multiple benefits; patients who received one had lower opioid use after surgery, lower pain scores, less nausea and vomiting after surgery, and shorter time in the hospital and in surgery, compared with patients who did not have a block. However, the patients who received a nerve block were also 3 times more likely to have a pain-related emergency department visit in the week after the procedure.
“It is good to confirm the benefits that regional anesthesia can provide these patients,” said lead author Edward Yap, MD, an anesthesiologist with The Permanente Medical Group and an adjunct investigator with the Kaiser Permanente Division of Research. “We need to explore further the reasons why they were more likely to have trouble managing their pain afterwards.”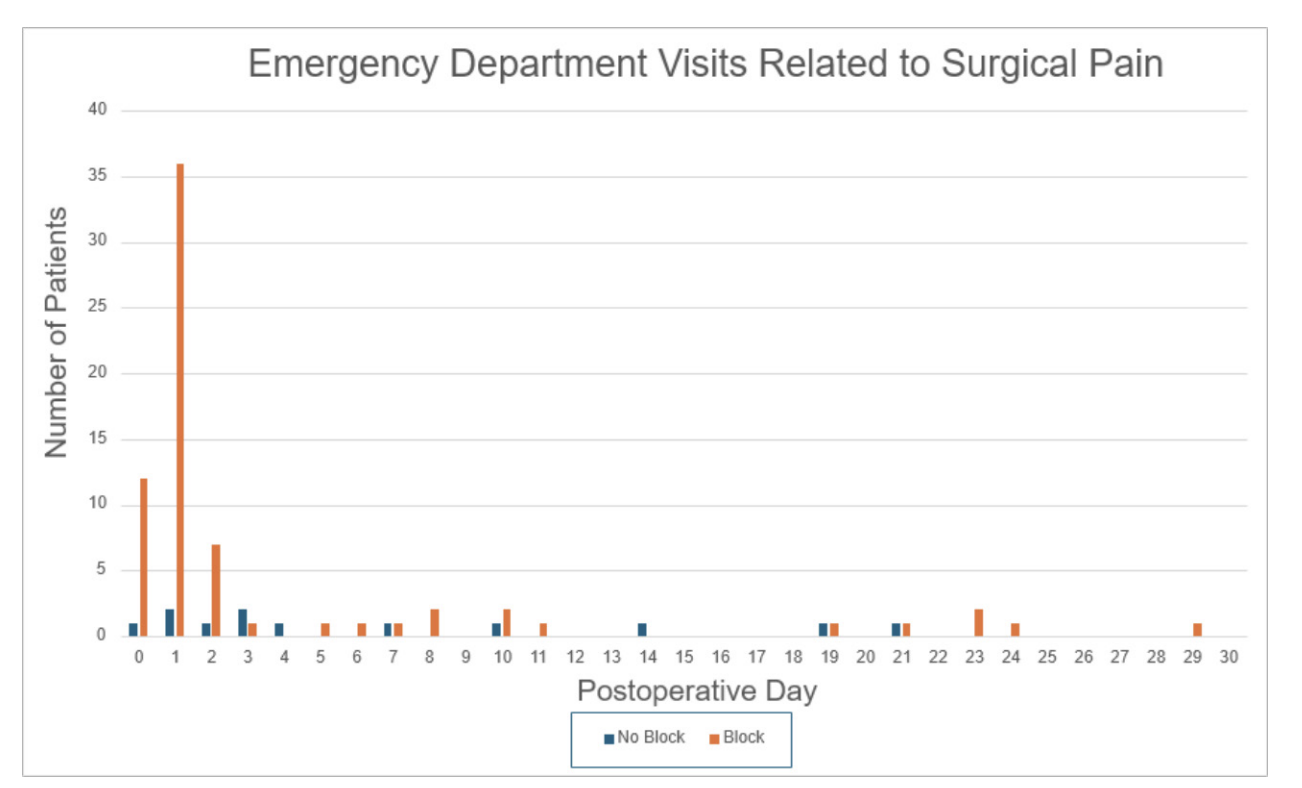
Anesthesiologists manage pain control — so the patient does not feel the procedure — and sedation, so the patient isn’t awake or doesn’t move while the surgeon is working. For surgery to repair a broken wrist, they typically choose between general anesthesia and opioids for sedation and pain control; or a nerve block combined with sedation.
Patients who don’t receive a nerve block, Yap said, are usually less likely to have chronic pain or other chronic health conditions, and less likely to take antidepressants.
The study’s results do not necessarily mean nerve blocks are not an effective choice, Yap said. Instead, they may suggest patients getting a nerve block need more guidance prior to surgery about the level of pain they may experience, and how best to manage it without seeking additional care.
“The nerve block does a good job numbing the pain for a period of time, but when that stops the patient may experience a sudden level of pain they aren’t expecting,” Yap said. “It may help to counsel patients in greater detail on this point before the procedure.”
Managing pain involves multiple factors, including the type of pain medication, whether the patient takes their prescribed medication, the patient’s overall health and individual response to pain medication, and patient expectations of how much pain they might have after an operation. “Pain is very personal and subjective,” Yap added.
Senior author Andrew Gray, MD, PhD, an anesthesiologist with the University of California, San Francisco said doctors could use the study’s insights in various ways. “Reducing return to care following surgery may be a matter of patient education to set expectations, using long-acting local anesthetic agents, and maintaining patient contact,” Gray said. “We now need studies to tease out the most important factors and identify the effective strategies for patients at high risk for pain.”

Co-author and hand surgeon David Zeltser, MD, said managing post-operative pain is a priority for both the anesthesiology team and orthopedic surgery team. “I have noticed that patients who receive a preoperative block have a smoother perioperative experience and generally the feedback I receive from them is positive,” said Zeltser, who practices with the Washington Permanente Medical Group. “But anecdotal data is not enough; we need carefully designed studies like this one to measure outcomes.”
Yap said he plans to extend this work to other outpatient orthopedic surgical procedures, examining how anesthetic choice, multimodal analgesia, and preoperative optimization shape recovery, pain, and downstream outcomes.
The study was supported by Kaiser Permanente Community Health.
Additional co-authors were Julia Wei, MPH, of the Kaiser Permanente Division of Research; Jonathan Khersonsky, MD, and Shin-I Lin, MD, of The Permanente Medical Group; and Kavenpreet S. Bal, MSc, of the Kaiser Permanente Bernard J. Tyson School of Medicine.
###
About the Kaiser Permanente Division of Research
The Kaiser Permanente Division of Research conducts, publishes, and disseminates epidemiologic and health services research to improve the health and medical care of Kaiser Permanente members and society at large. KPDOR seeks to understand the determinants of illness and well-being and to improve the quality and cost-effectiveness of health care. Currently, DOR’s 720-plus staff, including 73 research and staff scientists, are working on nearly 630 epidemiological and health services research projects. For more information, visit divisionofresearch.kp.org.




Comments (0)