Kaiser Permanente study finds a mammography AI risk score used along with polygenic and clinical risk scores identifies more high-risk women
A risk model that combines a mammographic artificial intelligence (AI) risk score with polygenic and clinical risk scores more accurately identifies women at high risk of developing breast cancer than a clinical risk score used alone, a new Kaiser Permanente study found.

“Breast cancer risk tools can help identify high-risk women who are most likely to benefit from more frequent breast cancer screening or risk reduction with medications,” said lead author Vignesh Arasu, MD, PhD, a research scientist at the Kaiser Permanente Division of Research (DOR) and a radiologist with The Permanente Medical Group. “Our study shows that each of the 3 tests identifies a unique group of women, and that when all 3 risk tests are used we increase our ability to differentiate high-risk and low-risk women and provide more personalized screening recommendations.”
The study, published in the Journal of the National Cancer Institute, is one of the largest and most diverse to evaluate the ability of 3 scores — mammography AI, polygenic, and clinical — to predict breast cancer risk. It included 82,957 women enrolled between 2003 and 2020 in the Kaiser Permanente Research Bank, a national program that currently includes medical records, survey, and genetic data from more than 400,000 Kaiser Permanente members. All the women included in the study had a recent mammogram that showed no signs of breast cancer. None had a genetic mutation known to increase breast cancer risk or had previously been diagnosed with breast cancer.
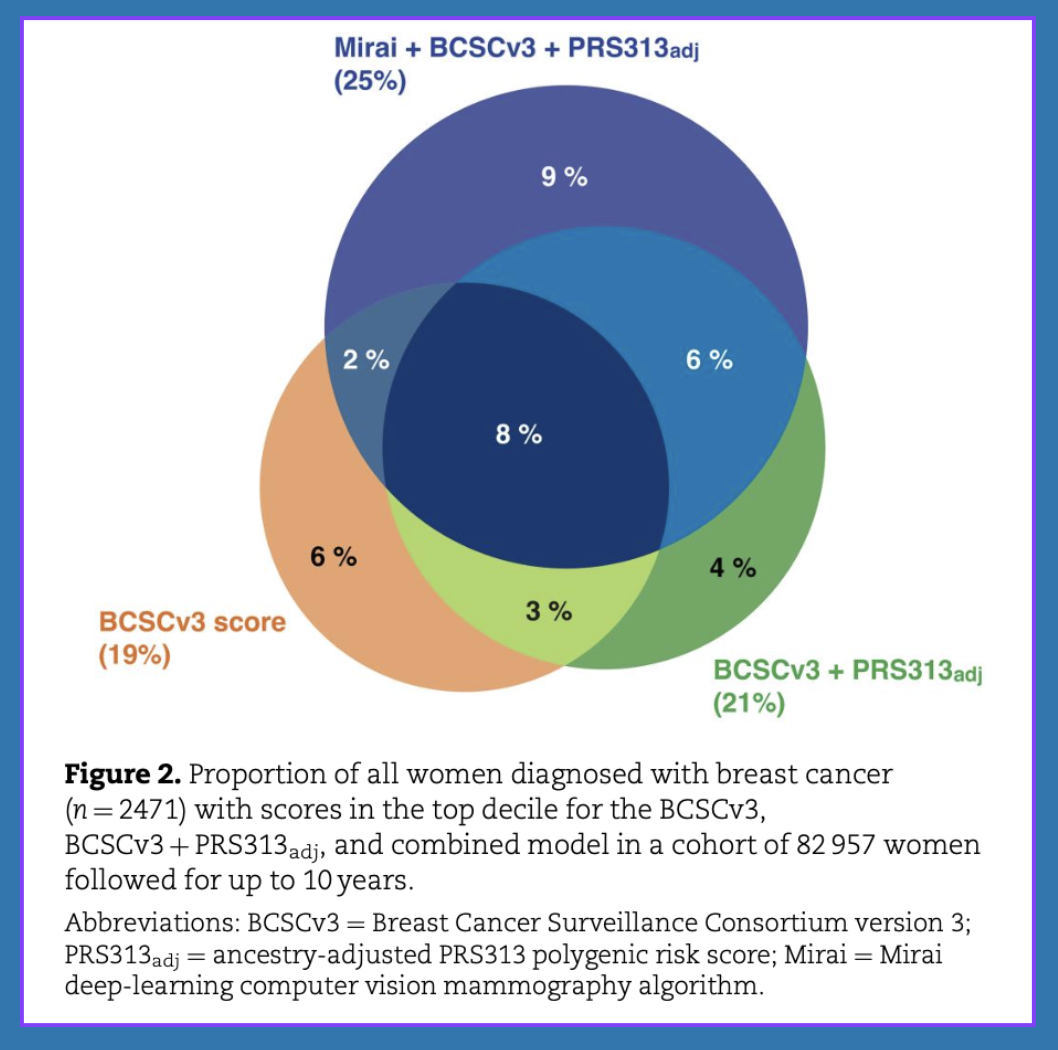
Over 10 years, 2,471, or 3%, of the women in the study were diagnosed with invasive breast cancer or ductal carcinoma in situ (DCIS). The risk model that incorporated all 3 risk assessment methods was the most accurate, with a C-index score of .70. (A score of .5 is equivalent to the flip of a coin; a score of 1.0 is perfect accuracy.) On its own, the clinical risk tool scored .62, while the polygenic test’s prediction accuracy was .61. Combining the clinical and polygenic risk scores resulted in a prediction accuracy of .66.

The study also found that among the women at highest risk of developing breast cancer, the clinical risk score alone identified 19% of the women who went on to develop breast cancer over a 10-year period while the combined model identified 26% of these women.
“From a modeling perspective, the key result is the consistent improvement in prediction accuracy when these risk scores are combined,” said study co-author Stacey E. Alexeeff, PhD, a research scientist and biostatistician at DOR. “We looked across different time horizons within the 10-year follow-up, and the combined model consistently performed better than each risk score alone.”
Advances in risk assessment
Clinical risk models have been used since 1989 to assess breast cancer risk; polygenic risk scores were introduced about 25 years later. Mammographic AI algorithms have been studied since 2022.
 The mammography AI algorithm predicts 5-year breast cancer risk based on the presence of risk-related imaging biomarkers it can detect on a mammogram. The clinical risk score considers factors such as age, race or ethnicity, family history of breast cancer, breast density, and body mass index. The polygenic risk score is determined by the presence or absence of 313 single nucleotide polymorphisms (SNPs) that prior studies have found to be associated with breast cancer.
The mammography AI algorithm predicts 5-year breast cancer risk based on the presence of risk-related imaging biomarkers it can detect on a mammogram. The clinical risk score considers factors such as age, race or ethnicity, family history of breast cancer, breast density, and body mass index. The polygenic risk score is determined by the presence or absence of 313 single nucleotide polymorphisms (SNPs) that prior studies have found to be associated with breast cancer.
The new study builds on a prior study led by Arasu that found AI mammography risk assessment was better at predicting future breast cancer risk than a clinical risk model.
“Our previous study showed that an AI risk score was slightly more accurate than a clinical risk score,” said Arasu. “This new study shows that by combining them, and by adding a polygenic risk score, we make a substantial improvement in accurately assessing risk.”
“As technologies for assessing risk continue to improve,” Arasu added, “we are likely to see even more improvement in our ability to predict risk.”
The study was funded by the National Cancer Institute and The Permanente Medical Group Delivery Science and Applied Research Program.
Co-authors include Tejomay Gadgil, MS, Ninah S. Achacoso, MS, Woodward Galbraith, Lawrence D. Gerstley, PhD, Lawrence H. Kushi, ScD, Amethyst D. Leimpeter, MS, Vincent Liu, MD, Ben J. Marafino, PhD, Lori C. Sakoda, PhD, MPH, Jun Shan, PhD, Marvella Villaseñor, MA, Mark Westley, Laurel A. Habel, PhD, and Cara L. Smith Gueye, PhD, MPH, of the Division of Research; Joseph H. Rothstein, MS, S. Taylor Head, PhD, Arjun Bhattacharya, PhD, and Weiva Sieh, MD, PhD, of the University of Texas; Jason B. Cord, MD, and Donald A. Lewis, of Kaiser Permanente Southern California; Laura J. Esserman, MD, Nola M. Hylton, PhD, Catherine Lee, PhD, Laura van’t Veer, PhD, and Jeffrey A. Tice, MD, of the University of California, San Francisco; Laurie R. Margolies, MD, Adriana Sistig, PhD, Li Shen, PhD, of the Icahn School of Medicine at Mount Sinai; Daniel A. Navarro, MD, The Permanente Medical Group; Albert Pu, MS, Kaiser Foundation Health Plan; Yiwey Shieh, MD, MAS, Weill Cornell Medicine; and Dorota J. Wisner, MD, Kaiser Permanente Northern California.
###
About the Kaiser Permanente Division of Research
The Kaiser Permanente Division of Research conducts, publishes, and disseminates epidemiologic and health services research to improve the health and medical care of Kaiser Permanente members and society at large. KPDOR seeks to understand the determinants of illness and well-being and to improve the quality and cost-effectiveness of health care. Currently, DOR’s 720-plus staff, including 73 research and staff scientists, are working on nearly 630 epidemiological and health services research projects. For more information, visit divisionofresearch.kp.org.




Comments (0)